
C1 Vertebral (Jefferson) Fracture
Summary:
-
A
C1 (atlas) vertebral fracture that usually occurs after an axial load injury
during a diving accident.
- When there are both anterior and posterior arch fractures this is called a "burst" fracture (also known as a Jefferson's fracture) and occurs when the occipital condyles are forced into the lateral masses of C1.
- While neurologic deficits may not always exist on presentation, imaging of the vertebral arteries is important due to concerns for late-onset neurologic deficits caused by blood flow disruptions.
- There are 2 classifications for the different types of C1 fractures which are listed below.
C1 Vertebral Fractures
|
|---|
-
C1 vertebral fractures primarily occur because the occipital condyles of the skull are forced into the lateral masses of C1.
- Unless there is retropulsed fragment of bone, patients usually do not have a
spinal cord injury or neurologic deficits because the fracture spread outward
or radially.
- However, the vertebral arteries are at high risk of injury (dissection and/or thrombosis) or spasm due to inflammation which can result in neurologic deficits.
- Landell and Van Peteghem Classification:
- Type 1 = Fracture of either the anterior or posterior arches (but not both)
- Type 2 = Fractures of both anterior and posterior arches (i.e., a burst fracture)
- Type 3 = Fracture involving the lateral masses of C1
- Jefferson Classification:
- Type 1 = Fracture of the posterior arch only
- Type 2 = Fracture of the anterior arch only
- Type 3 = Fracture of both the anterior and posterior arches (i.e., a burst or Jefferson's fracture)
- Type 4 = Fracture of the lateral mass(es) of C1
- Note:
- The clinician should assess for vertebral artery injuries with a CTA of the neck.
If a vertebral artery dissection is found, the patient will need anticoagulation
with heparin and further evaluation by interventional radiology.
- Assuming the atlantodens interval (ADI) is not widened or an MRI does not show disruption of the transverse ligament, the patient can be managed with a cervical spine collar. Otherwise the patient may need to be put into a halo immobilizer and undergo posterior C1-C2 lateral mass internal fixation.
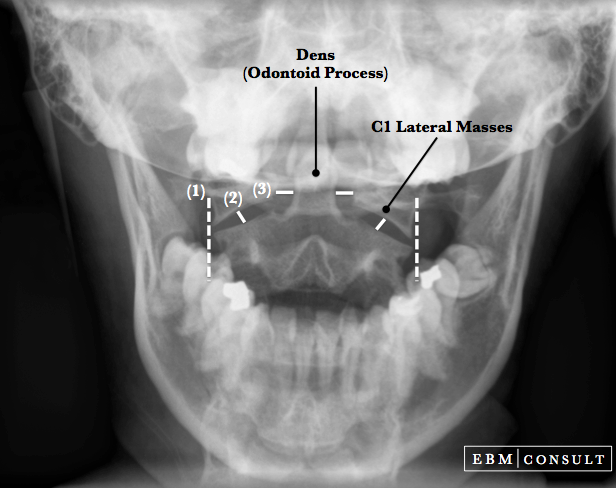
- Open Mouth Odontoid
Radiograph:
- Reveals asymmetry of the
spaces between the dens (located on C2 and projecting up) and the lateral
masses of C1.
- The lateral masses are usually extended out laterally with respect to the margins of C2 because the C1
fragments spread radially.
- CT Scan & MRI:
- Both imaging modalities can help
to determine if the fracture line involves both the anterior and posterior
arches, but an MRI can more useful and provide more information on local
soft-tissue injury (such as pre-vertebral hemorrhage or swelling) as well as
ligamentous injury.
- Given the mechanism of injury, a CT angiogram of the neck should be considered, especially if there are new neurologic deficits present.
- Jefferson G. Br J Surg 1919;7(27):407-22.
- Landells CD et al. Fractures of the atlas: classification, treatment and morbidity. Spine 1988;13(5):450-2. PubMed
- Miyachi S et al. Cerebellar stroke due to vertebral artery occlusion after cervical spine trauma. Two case reports. Spine
1994;19(1):83-8. PubMed
- Muratsu H et al. Cerebellar infarction resulting from vertebral artery occlusion associated with a Jefferson fracture. J Spinal Disord Tech 2005;18(3):293-6. PubMed
- Kontautas E et al. Management of acute traumatic atlas fractures. J Spinal Disord Tech 2005;18:402-5.

Mechanism of Injury
Classifications of C1 Fractures
There are 2 main classification systems for C1 vertebral fractures.
Imaging Considerations
Related Content
To see other related content click or tap on an item below:
Dens Fractures Lateral C-Spine Odontoid View
Rerferences



