Vitamin
B12 is a well known water soluble vitamin necessary for a number of metabolic
reactions and prevention of certain medical complications, most commonly
hematopoietic disorders and spinal cord related neuropathies (additional
details to these disorders will be summarized in future publications).1,2
Vitamin B12 is also known as cobalamin or cyanocobalamin (the form found in
most over the counter supplements).1 It gets its name in part due to its
chemical structure since it contains cobalt, thus the reason it is known
as cobalamin.1 As with any vitamin, human beings cannot
synthesize or produce their own vitamins and thus must obtain them from dietary
sources, bacteria making up our normal flora, and/or through supplements.
As such, vitamins are "vital to life".
As
it relates to the need for vitamin B12, the molecular state in which the
vitamin B12 is introduced into the body can impact how efficient it can be
absorbed from a normally functioning gastrointestinal tract. Vitamin B12
bound to protein in foods must undergo an initial or early separation reaction
before it can be absorbed in the ileum of the small intestine, whereas most
forms found in supplements do not undergo this separation reaction as they are
already in the free form. Recognizing this difference becomes important
in future publications related to drug interactions and their clinical
context. For now, the following concisely describes the sequence of
events that must take place for vitamin B12 to get into the body.
If
vitamin B12 is ingested in its free (or nonprotein bound form), it will bind to
a carrier protein known as R-binders or transcobalamin I that is secreted by
both the salivary glands in the oropharynx and the gastric mucosal cells within
the stomach (see figure 1 below).1,2 The free vitamin B12 ingested by
mouth will remain in the bound form with an R-binder until it reaches the
second segment of the duodenum in the small intestine.
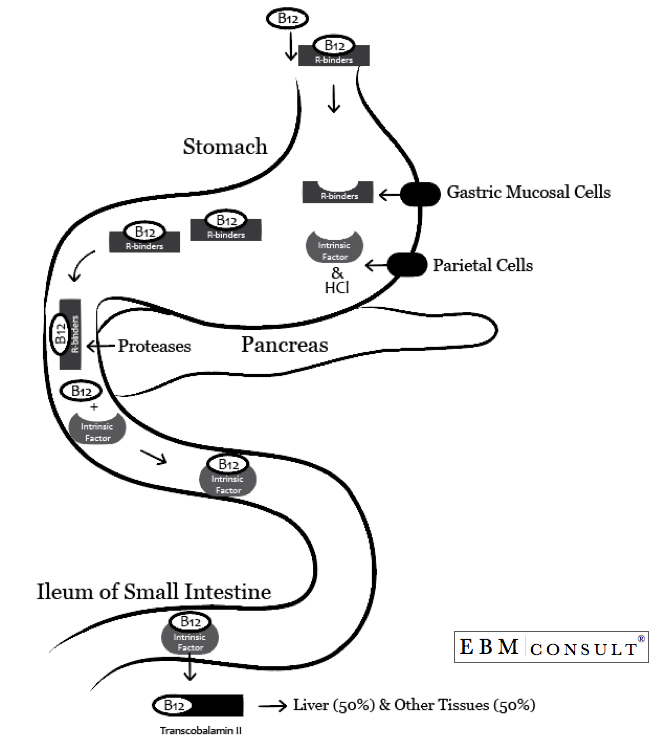
If
the vitamin B12 is ingested in its protein bound form, then it must first
undergo a proteolytic cleavage in the stomach or duodenum where it will bind to
an R-binder and then enter into the duodenum for further cleavage.1,2
This proteolytic cleavage is mostly dependent on the functional activity of
pepsin. As a reminder, the chief cells within the stomach will secrete
the pepsinogen into the lumen of the stomach. The presence of the
hydrochloric acid also provided by the parietal cells is necessary to convert
the pepsinogen to pepsin. The functionally active pepsin can then degrade
the newly ingested protein source holding onto to the vitamin B12. Upon
this protein degradation, the free vitamin B12 will then proceed as above to be
bound to an R-binder or transcobalamin I for entry into the duodenum.
Therefore, regardless of the molecular state of vitamin B12 ingested, it is
mostly delivered to the duodenum as a complex with an R-binder.
Intrinsic
factor is also present in the gastric and intestinal contents that contain the
vitamin B12 complexed to R-binders and being delivered to the duodenum.
In addition to the hydrochloric acid secreted from the stomach, the properly
functioning parietal cells also secrete intrinsic factor, however nothing is
bound to the intrinsic factor at this point. Upon entry into the second
segment of the duodenum, the pancreas will secrete additional protease, which
will then degrade the R-binders holding onto the vitamin B12. It is at
this point the vitamin B12 will bind to (or complex with) intrinsic factor for
the remainder of its journey to the ileum of the small intestine for
absorption.
Assuming
a functionally intact ileum, the vitamin B12/intrinsic factor complex is taken
up into the enterocyte at this point in the small intestine. The absorbed
vitamin B12 then binds to transcobalamin II where approximately 50% of the
vitamin B12 will be delivered to the liver and the remainder will be delivered
to other tissues. In fact, the liver's storage of vitamin B12 is
significant enough that it could take a year or more before deficiency of
vitamin B12 manifests into clinically relevant pathology.
References:
- Lieberman M, Marks AD. Tetrahydrofolate, Vitamin B12, and
S-adenosylmethionine. Lieberman M, Marks AD. Eds. In: Mark's Basic
Medical Biochemistry: A Clinical Approach. 3rd Ed. Wolters Kluwer/Lippincott Willaims & Wilkins. Philadelphia, PA. 2009.
- Institute
of Medicine. Food and Nutrition Board. Dietary Reference Intakes:
Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12,
Pantothenic Acid, Biotin, and Choline. Washington, DC: National Academy
Press, 1998.




