
Lachman Test: Physical Exam
|
|---|
-
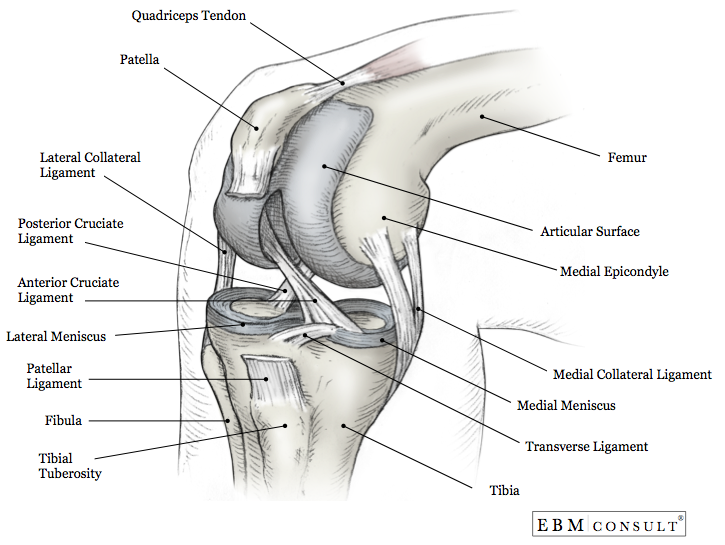
The ACL attaches to the anterior intercondylar
area of the tibia then passes posteriorly, laterally, and upward to attach to
the femur on the medial side of its lateral condyle.
- The ligament prevents forward sliding of the tibia on the femur and prevents hyperextension of the knee.
- The patient should by relaxed and lying supine on the exam
table, heel on the table and knee flexed 20°-30 °.
- The examiner should stand to
the side of the exam table.
- Hold the femur firmly with one hand to prevent
motion of the upper leg and relax the hamstrings.
- Place the thumb of the other
hand on the anterior side of the tibia and grasp the posterior side of the
tibia near the joint line with the fingers.
- Apply a brisk posterior-to-anteriorly force through the tibia (tug forward).
- Positive:
- Np distinct endpoint is felt by examiner and there is increased translation of the tibia (excessive movement).
- Patients with a torn PCL may test positive with a Lachman test (tibia will rest further posterior than usual due to the absence of the PCL).
- Negative:
- Distinct endpoint is felt by examiner.
- Acute:
- Sensitivity: 0.94
- Specificity: 0.97
- Chronic:
- Sensitivity: 0.95
- Specificity: 0.9
- Likelihood Ratios:
- Positive test: 42.0 (95% CI, 2.7-651)
- Negative test: 0.1 (95% CI, <0.0-0.4)
- It is important to obtain/maintain the correct joint angle
(20° to 30°) because a position closer to full extension has less anterior
translation of the tibia and can result in a false endpoint.
- The ACL is more
maximally stressed at 20° and can be assessed more accurately due to other
tissues not limiting anterior translation of the tibia.
- The integrity of the PCL should be assessed prior to looking at ACL integrity.
- Benjaminse A et al. "Clinical diagnosis of an anterior
cruciate ligament rupture: a meta-analysis." The Journal of orthopaedic
and sports physical therapy. May 2006; 36(5):267-288.
- Bickley LS et al. Bates' Guide to Physical Examination and
History Taking. 11th ed. Philadelphia, PA: Lippincott Williams & Wilkins.
2013;658.
- Manske, Robert. Post-surgical Orthopedic Sports Rehabilitation: Knee
and Shoulder. St. Louis, MO: Mosby Elsevier, 2006. 46-7.
- Marieb EN, Hoehn K. Anatomy & Physiology. 3rd ed. San Fransisco, CA: Pearson Benjamin Cummings. 2008;237.
- Orient, JM. Sapira's Art and Science of Bedside Diagnosis. 4th ed.
Philadelphia, PA: Lippincott Williams & Wilkins. 2010;513-4.
- Solomon DH et al. The rational clinical examination. Does this patient have a torn meniscus or ligament of the knee? Value of the physical examination. JAMA. 2001;286(13):1610-20.
Anatomy
Technique
Results
Diagnostic Accuracy
Pearls
References



