-
Numerous genetic polymorphisms of
adrenergic receptors have been identified. The most common genetic variants in
humans are referred to as single nucleotide polymorphisms (SNPs). Although many
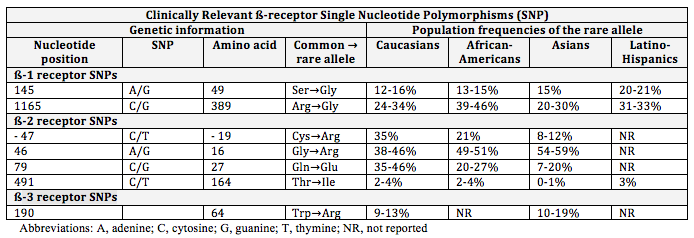
SNPs have been discovered in beta-receptors, few are clinically relevant. There
are 2 clinically relevant SNPs for the beta 1-receptors (Ser49Gly and
Arg389Gly), 4 for the beta 2-receptors (Cys-19Arg, Arg16Gly, Gln27Glu,
Thr164Ile), and 1 for the beta 3-receptors (Trp64Arg).1 Frequently,
polymorphisms occur in certain combinations labeled haplotypes. Results
are controversial, but there is data to support a relationship between
ß-receptor SNPs and outcomes. Understanding the functional consequences
of specific polymorphisms leads to the individualization of drug therapy based
on a patient's genetic makeup and could explain distinct inter-individual
variability.
The table below summarizes
clinically relevant ß-receptor polymorphisms, with an emphasis on the specific
location of genetic mutations and the populations primarily affected.2-10
ß1- receptor polymorphisms
The most
clinically relevant SNPs for ß1-receptors include Ser49Gly and Arg389Gly. Ser49Gly leads to impaired down-regulation of
the beta-1 receptor, and Arg389Gly leads to higher signal transduction.11, 12 Therefore, carriers of either variant have
enhanced ß1-receptor activity and are more sensitive to beta-blocker therapy.
ß2-receptor polymorphisms
The most clinically relevant SNPs for ß2-receptors include
Arg16Gly, Gln27Glu, and Cys-19Arg. Receptors
with the Gly16 variant have enhanced down-regulation of the beta-2 receptor. In contrast, receptors with the Glu27 variant appear
resistant to down-regulation.3 Finally,
the Cys-19 variant is associated with increased beta-2 receptor expression.8
These
polymorphisms of beta-receptors alter the sensitivity of patients to drug
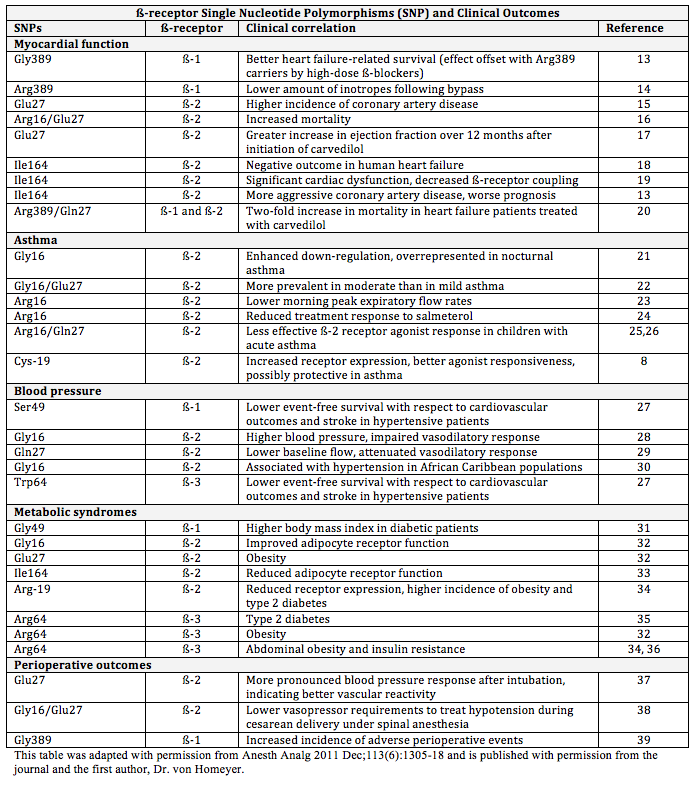
therapy, changing the pharmacodynamics of drug response. Table 2 discusses clinical outcomes as they
relate to each ß-receptor polymorphism.
Although
the known and studied polymorphisms of beta-receptors do not seem to produce
disease, it is evident these genetic mutations can play a role in risk for
disease and disease modification. Moreover, the polymorphisms may change
how a patient responds to drug therapy, specifically beta-agonist and
antagonist therapies. Such genotypic analysis can help guide drug
selection and dosing. Although somewhat controversial, the evidence from
research continues to improve understanding of beta-receptor signaling.
There is a great need for large, randomized, controlled trials to evaluate the
conflicting data related to beta-receptor SNPs and related differences
regarding disease and medications. Recent studies suggest that analysis
of haplotype may be more beneficial than analysis of individual polymorphisms
in relation to drug response. These trials should by multinational and
include a variety of ethnicities. Future pharmacogenetic evidence will
promote the practice of personalized medicine.
References:
-
von
Homeyer P, Schwinn D. Pharmacogenomics of ß-adrenergic Receptor Physiology and
Response to ß-Blockade. Anesth Analg 2011 Dec;113(6):1305-18. Epub 2011 Sep
29.
-
Moore
JD, Mason DA, Green SA, Hsu J, Liggett, SB. Racial differences in the
frequencies of cardiac ß1-adrenergic receptor polymorphisms: analysis of
c145A>G and c1165G>C. Hum Mutat 1999;14,271.
-
Small
KM, McGraw DW, Liggett SB. Pharmacology and physiology of human adrenergic
receptor polymorphisms. Annu Rev Pharmacol Toxicol 2003;43: 381−411.
-
Kirstein
SL, Insel PA. Autonomic nervous system pharmacogenomics: a progress report.
Pharmacol Rev 2004;56,31−52.
-
Taylor
MR, Bristow MR. The emerging pharmacogenomics of the β-adrenergic receptors.
Congest Heart Fail 2004;10, 281−8.
-
Pacanowski
MA, Johnson JA. PharmGKB submission update: IX. ADRB1 gene summary. Pharmacol
Rev 2007;59,2−4.
-
Xie
HG, Dishy V, Sofowora G, Kim RB, Landau R, Smiley RM, et al. Arg389Gly
β1-adrenoceptor polymorphism varies in frequency among different ethnic groups
but does not alter response in vivo. Pharmacogenetics 2001; 11, 191−7.
-
McGraw
DW, Forbes SL, Kramer LA, Liggett SB. Polymorphisms of the 5' leader cistron of
the human beta 2- adrenergic receptor regulate receptor expression J Clin
Invest 1998;102:1927-32.
-
Xie
HG, Stein CM, Kim RB, Xiao ZS, He N, Zhou HH, et al. Frequency of functionally
important beta-2 adrenoceptor polymorphisms varies markedly among
African-American, Caucasian, and Chinese individuals. Pharmacogenetics
1999; 9, 511−16.
-
Maxwell
TJ, Ameyaw MM, Pritchard S, Thornton N, Folayan G, Githanga J, et al. Beta-2
adrenergic receptor genotypes and haplotypes in different ethnic groups. Int J
Mol Med 2005;16, 573−80.
-
Rathz
DA, Brown KM, Kramer LA, Liggett SB. Amino acid 49 polymorphisms of the human
beta1-adrenergic receptor affect agonist-promoted trafficking. J Cardiovasc
Pharmacol 2009; 39, 155-60.
-
Mason
DA, Moore JD, Green SA, Liggett SB. A gain-of-function polymorphism in a
G-protein coupling domain of the human beta1-adrenergic receptor. J Biol Chem
2009; 274,12670-4.
-
Biolo
A, Clausell N, Santos KG, Salvaro R, Ashton-Prolla P, Borges A, Rohde LE.
Impact of beta-1 adrenergic receptor polymorphisms on susceptibility to heart
failure, arrhythmogenesis, prognosis, and response to beta-blocker therapy. Am
J Cardiol 2008;102:726-32.
-
Leineweber
K, Bogedain P, Wolf C, Wagner S, Weber M, Jakob HG, Heusch G, Philipp T, Brodde
OE. In patients chronically treated with metoprolol, the demand of inotropic
catecholamine support after coronary artery bypass grafting is determined by
the Arg389Gly-beta 1-adrenoceptor polymorphism. Naunyn Schmiedebergs Arch Pharmacol
2007; 375:303-9.
-
Barbato
E, Berger A, Delrue L, Van Durme F, Manoharan G, Boussy T, Heyndrickx GR, De
Bruyne B, Ciampi Q, Vanderheyden M, Wijns W, Bartunek J. GLU-27 variant of beta
2- adrenergic receptor polymorphisms is an independent risk factor for coronary
atherosclerotic disease. Atherosclerosis 2007;194:e80-6.
-
Lanfear
DE, Jones PG, Marsh S, Cresci S, McLeod HL, Spertus JA. Beta-2 adrenergic
receptor genotype and survival among patients receiving beta-blocker therapy
after an acute coronary syndrome. JAMA 2005;294:1526-33.
-
Metra
M, Covolo L, Pezzali N, Zaca V, Bugatti S, Lombardi C, Bettari L, Romeo A,
Gelatti U, Giubbini R, Donato F, Dei Cas L. Role of beta-adrenergic receptor
gene polymorphisms in the long-term effects of beta-blockade with carvedilol in
patients with chronic heart failure. Cardiovasc Drugs Ther 2010;24:49-60.
-
Liggett
SB, Wagoner LE, Craft LL, Hornung RW, Hoit BD, McIntosh TC, Walsh RA. The
Ile164 beta 2-adrenergic receptor polymorphism adversely affects the outcome of
congestive heart failure. J Clin Invest 1998;102:1534-9.
-
Turki
J, Lorenz JN, Green SA, Donnelly ET, Jacinto M, Liggett SB. Myocardial
signaling defects and impaired cardiac function of a human beta 2-adrenergic
receptor polymorphism expressed in transgenic mice. Proc Natl Acad Sci USA
1996;93:10483-8.
-
Petersen
M, Andersen JT, Hjelvang BR, Broedbaek K, Afzal S, Nyegaard M, Borglum AD,
Stender S, Kober L, Torp Pedersen C, Poulsen HE. Association of beta-adrenergic
receptor polymorphisms and mortality in carvedilol-treated chronic heart
failure patients. Br J Clin Pharmacol 2011;71:556-65.
-
Turki
J, Pak J, Green SA, Martin RJ, Liggett SB. Genetic polymorphisms of the beta
2-adrenergic receptor in nocturnal and non-nocturnal asthma. Evidence that
Gly16 correlates with the nocturnal phenotype. J Clin Invest
1995;95:1635-41.
-
Weir
TD, Mallek N, Sandford AJ, Bai TR, Awadh N, Fitzgerald JM, Cockcroft D, James
A, Liggett SB, Pare PD. Beta 2-adrenergic receptor haplotypes in mild, moderate
and fatal/near fatal asthma. Am J Respir Crit Care Med 1998;158:787-91.
-
Israel
E, Chinchilli VM, Ford JG, Boushey HA, Cherniack R, Craig TJ, Deykin A, Fagan
JK, Fahy JV, Fish J, Kraft M, Kunselman SJ, Lazarus SC, Lemanske RF Jr, Liggett
SB, Martin RJ, Mitra N, Peters SP, Silverman E, Sorkness CA, Szefler SJ,
Wechsler ME, Weiss ST, Drazen JM. Use of regularly scheduled albuterol
treatment in asthma: genotype stratified, randomised, placebo-controlled
cross-over trial. Lancet 2004;364:1505-12.
-
Wechsler
ME, Lehman E, Lazarus SC, Lemanske RF Jr, Boushey HA, Deykin A, Fahy JV,
Sorkness CA, Chinchilli VM, Craig TJ, DiMango E, Kraft M, Leone F, Martin RJ,
Peters SP, Szefler SJ, Liu W, Israel E. Beta-adrenergic receptor polymorphisms
and response to salmeterol. Am J Respir Crit Care Med 2006;173:519-26.
-
Carroll
CL, Stoltz P, Schramm CM, Zucker AR. Beta 2- adrenergic receptor polymorphisms
affect response to treatment in children with severe asthma exacerbations.
Chest 2009;135:1186-92.
-
Martin
AC, Zhang G, Rueter K, Khoo SK, Bizzintino J, Hayden CM, Geelhoed GC, Goldblatt
J, Laing IA, Le Souef PN. Beta 2-adrenoceptor polymorphisms predict response to
beta 2-agonists in children with acute asthma. J Asthma 2008;45:383-8.
-
Iwamoto
Y, Ohishi M, Yuan M, Tatara Y, Kato N, Takeya Y,Onishi M, Maekawa Y, Kamide K,
Rakugi H. Beta-adrenergic receptor gene polymorphism is a genetic risk factor
for cardiovascular disease: a cohort study with hypertensive patients.
Hypertens Res 2011;34:573-7.
-
Hoit
BD, Suresh DP, Craft L, Walsh RA, Liggett SB. Beta2-adrenergic receptor polymorphisms
at amino acid 16 differentially influence agonist-stimulated blood pressure and
peripheral blood flow in normal individuals. Am Heart J 2000;139:537-42.
-
Cockcroft
JR, Gazis AG, Cross DJ, Wheatley A, Dewar J, Hall IP, Noon JP. Beta(2)-adrenoceptor
polymorphism determines vascular reactivity in humans. Hypertension
2000;36:371-5.
-
Kotanko
P, Binder A, Tasker J, DeFreitas P, Kamdar S, Clark AJL, Skrabal F, Caulfield
M. Essential hypertension in African Caribbean associates with a variant of the
beta(2)-adrenoceptor. Hypertension 1997;30:773-6.
-
Nonen
S, Yamamoto I, Liu JM, Maeda M, Motomura T, Igarashi T, Fujio Y, Azuma J.
Adrenergic beta (1) receptor polymorphism (Ser49Gly) is associated with obesity
in type II diabetic patients. Biol Pharm Bull 2008;31:295-8.
-
Large
V, Hellstrom L, Reynisdottir S, Lonnqvist F, Eriksson P, Lannfelt L, Arner P.
Human beta-2 adrenoceptor gene polymorphisms are highly frequent in obesity and
associate with altered adipocyte beta-2 adrenoceptor function. J Clin Invest 1997;100:3005-13.
-
Hoffstedt
J, Iliadou A, Pedersen NL, Schalling M, Arner P. The effect of the beta (2)
adrenoceptor gene Thr164Ile polymorphism on human adipose tissue lipolytic
function. Brit J Pharmacol 2001;133:708-12.
-
Yamada
K, Ishiyama-Shigemoto S, Ichikawa F, Yuan XH, Koyanagi A, Koyama W, Nonaka K.
Polymorphism in the 5'- leader cistron of the beta (2)-adrenergic receptor gene
associated with obesity and type 2 diabetes. J Clin Endocr Metab
1999;84:1754-7.
-
Gjesing
AP, Andersen G, Borch-Johnsen K, Jorgensen T, Hansen T, Pedersen O. Association
of the beta 3-adrenergic receptor Trp64Arg polymorphism with common metabolic
traits: studies of 7605 middle-aged white people. Mol Genet Metab 2008;94:90-7.
-
Widen
E, Lehto M, Kanninen T, Walston J, Shuldiner AR, Groop LC. Association of a
polymorphism in the beta 3-adrenergic-receptor gene with features of the
insulin resistance syndrome in Finns. N Engl J Med 1995;333:348-51.
-
Kim
NS, Lee IO, Lee MK, Lim SH, Choi YS, Kong MH. The effects of beta 2
adrenoceptor gene polymorphisms on vasopressor response during laryngoscopy and
tracheal intubation. Anaesthesia 2002;57:227-32.
-
Smiley
RM, Blouin JL, Negron M, Landau R. Beta 2- adrenoceptor genotype affects
vasopressor requirements during spinal anesthesia for cesarean delivery.
Anesthesiology 2006;104:644-50.
-
Zaugg
M, Bestmann L, Wacker J, Lucchinetti E, Boltres A, Schulz C, Hersberger M,
Kalin G, Furrer L, Hofer C, Blumenthal S, Muller A, Zollinger A, Spahn DR,
Borgeat A. Adrenergic receptor genotype but not perioperative bisoprolol
therapy may determine cardiovascular outcome in at-risk patients undergoing
surgery with spinal block: the Swiss Beta Blocker in Spinal Anesthesia (BBSA)
study: a double-blinded, placebo-controlled, multicenter trial with 1 year
follow-up. Anesthesiology 2007;107:33-44.
|




