
Otoscope Examination
|
|---|
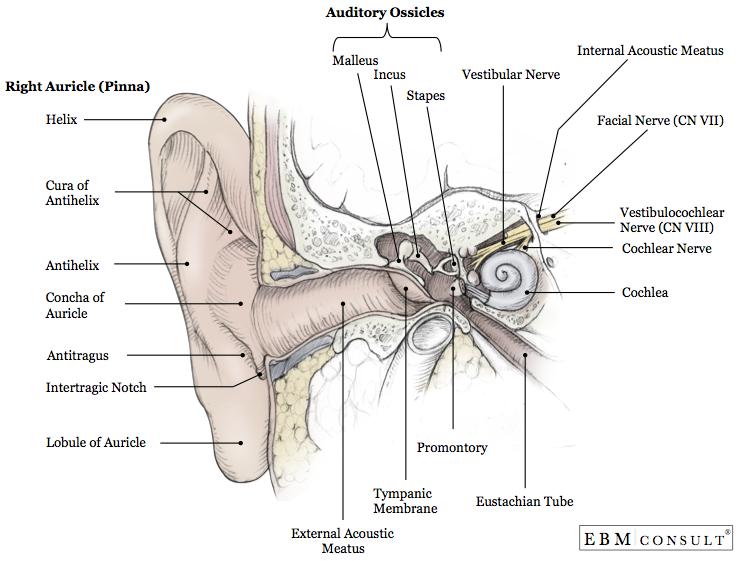
- The external auditory canal (EAC) curves inward and is approximately 24 mm long. Cartilage surrounds the outer portion and the skin is hairy and contains glands that produce cerumen. The inner portion is surrounded by bone and lined with thin, hairless skin
- In infants, the EAC is directed upward and backward from the outside
- The EAC curves downward and forward in children >3 years of age
- The tympanic membrane (TM) lies at the at the end of the EAC and marks the lateral limit of the external ear
- The external ear captures sound waves for transmission into the middle/inner ear
- The patient should be sitting on the exam table
- Position the patient's head so you can see comfortably through the instrument
- Grasp the auricle and firmly but gently pull it upward, backward, and slightly away from the head (straightens the EAC, should be painless)
- Turn the otoscope light on and hold the handle between your thumb, index finger, and middle finger and point the handle upward or laterally
- Brace your hand against the patient's temple/cheek using your fourth and fifth fingers to stabilize the otoscope and guard against trauma with sudden movements
- Direct the speculum in a slightly downward fashion as you insert it into the EAC approximately 0.25 to 0.5 inches
- Remove cerumen, discharge, debris, or foreign bodies if inhibiting direct visualization of the TM
- Inspect the walls of the EAC
- Carefully move the speculum to see as much of the TM as possible
- Inspect the TM for color, translucency, vascularity and position
- Identify the umbo, manubrium of the malleus, the light reflex, the pars flaccida, and the pars tensa
- Use a pneumatic otoscope to assess the TM mobility
- Insert the pneumatic otoscope into the ear canal and ensure an airtight seal (failure to obtain a seal can produce a false-positive/lack of movement finding)
- Squeeze the bulb to introduce air into the canal (the TM and its light reflex should move inward) being careful not to apply excessive pneumatic pressure
- Release the bulb to remove air (TM should move outward)
- Have the child sit in the parents lap or lie down on their side, back, or abdomen with the ear to be examined facing upwards
- If lying down, have the parent hold the arms either extended or close to the sides to limit motion
- If sitting, place the child's legs between the parents legs and have the parent place one arm around the child's body and use the other hand to hold the child's head firmly against the parent's chest
- Grasp the auricle with your thumb and forefinger of your nondominant hand and pull to straighten the canal
- The EAC curves upward in infants so pull down and back to the 6 to 9 o'clock range
- The EAC curves downward and forward in children >3 years of age so pull up and back toward a 10 o'clock position
- Insert the speculum into the meatus between the 3 and 9 o'clock positions in a downward and forward position no more than 0.23-0.5 inches (in older children)
- In neonates and infants, the 2 mm speculum may need to be inserted deeper due to the underdeveloped cartilaginous and bony structures
- Continue steps 4-11 listed above
- Use the largest ear speculum that the canal will accommodate (allows better visualization of the TM)
- Insertion of the speculum into the posterior/bony portion of the EAC causes pain and may damage the delicate skin of the canal
- Do not lavage the canal if a perforated eardrum is suspected
- Ensure the water/fluid for lavage is approximately body temperature as cold/hot fluids will induce nystagmus and/or vomiting
- Changing the air pressure in the EAC with the pneumatic otoscope may elicit a painful response in acute otitis media
- Bickley LS et al. Bates' Guide to Physical Examination and History Taking. 11th ed. Philadelphia, PA: Lippincott Williams & Wilkins. 2013;232-6, 834-5.
- Hockenberry MJ, Wilson D. Wong's Essentials of Pediatric Nursing. 8th ed. St. Louis, MO: Mosby Elsevier. 2009; 138-40.
- Orient, JM. Sapira's Art and Science of Bedside Diagnosis. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins. 2010; 226-7.
Anatomy
Technique
Technique (Adult)
Technique (Child)
Notes
References



