
Physical Exam: Anterior Drawer Test
|
|---|
-
The
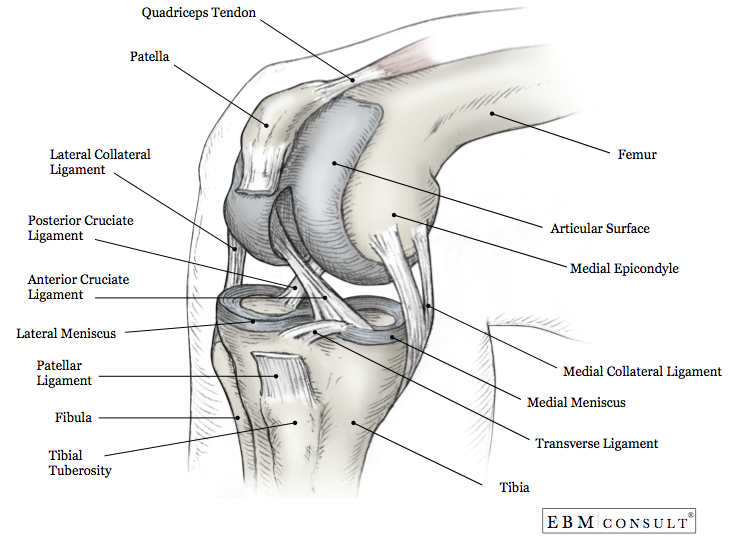
ACL attaches to the anterior intercondylar area of the tibia then passes
posteriorly, laterally, and upward to attach to the femur on the medial side of
its lateral condyle.
- The ligament prevents forward sliding of the tibia on the femur and prevents hyperextension of the knee.
- The patient should be lying supine on the exam table
- Have the patient flex the hip and knees to 90°, feet should be flat on the table (the examiner may sit on the patients foot to ensure it stays flat)
- Cup your hands around the knee with the thumbs on the medial and lateral joint line and the fingers on the medial and lateral insertions of the hamstring
- Apply an posterior-to-anterior directed force through
the superior tibia to draw the tibia forward toward you
- Observe if the tibia slides forward (like a drawer) from under the femur
- Repeat the test on the other leg, comparing the degree of forward movement
- Positive Test:
- The tibia jerks forward showing the contours of the upper tibia and includes the lack of an end-feel or excessive translation
- An ACL tear is 11.5 times more likely
- Negative Test:
- Little movement is noted
- A few degrees of forward movement are normal if equally present on both sides
- Summary: The anterior drawer test appears to be a specific test when ruling in a torn ACL when the test is positive and the sensitivity and specificity appear to be better for chronic conditions.
- Acute:
- Sensitivity = 49%
- Specificity = 58%
- Chronic:
- Based on a meta-analysis of 28 studies (Benjaminse et al), the anterior drawer test shows sensitivity and specificity, however there was heterogeneity in the studies included:
- Sensitivity = 92% (95% CI, 88 - 95%)
- Specificity = 91% (95% CI, 87 - 94%)
- Likelihood ratios:
- Positive exam: LR = 3.8 (95% confidence interval [CI], 0.7 - 22.0)
- Negative exam: LR = 0.30 (95% CI, 0.05 - 1.50)
- Performing the test with the foot internally rotated further isolates the ACL
- Synthesis of a group of examination maneuvers and historical items may be required for adequate diagnosis (the composite examination for specific ligamentous injuries of the knee performed much better than specific maneuvers)
- Benjaminse
A et al. "Clinical diagnosis of an anterior cruciate ligament rupture: a
meta-analysis." J Ortho Sports Phys Ther 2006;36(5):267-288. PubMed
- Solomon DH et al. The rational clinical examination. Does this patient have a torn meniscus or ligament of the knee? Value of the physical examination. JAMA. 2001;286(13):1610-20. PubMed
- Bickley LS et al. Bates' Guide to Physical Examination and History Taking. 11th ed. Philadelphia, PA: Lippincott Williams & Wilkins. 2013;658.
- Marieb EN, Hoehn K. Anatomy & Physiology. 3rd ed. San Fransisco, CA: Pearson Benjamin Cummings. 2008;237.
- McGee S. Examination of the musculoskeletal system - the shoulder. Ch 53. In Evidence-Based Physical Diagnosis, 2nd ed. St. Louis: Saunders, 2007.
- Orient, JM. Sapira's Art and Science of Bedside Diagnosis. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins. 2010;512-3.
Anatomy
Physical Exam Technique
Results
Diagnostic Accuracy
Pearls
References



